The 2026 Director of Public Health report
“Communities at the Centre: Creating better health together in Leeds”
Foreword
Welcome to the 2026 Director of Public Health Annual Report for Leeds. I’m delighted to share this report with you, which shows how we work with communities in Leeds to improve health and reduce health inequalities in our city.
This report draws on global evidence and our learning from working closely with communities across Leeds. It makes the case for embedding community-centred approaches at the heart of all our work to improve and protect the health of everyone in the city.
Leeds is a vibrant city, made up of many diverse communities with incredible strengths. These include 3,375 Voluntary, Community and Faith Sector (VCFS) organisations, over 200 languages spoken, vibrant faith communities, and beautiful green spaces that support health and wellbeing. However, as in every large city in the UK, there are long-standing inequalities between different communities. As a Marmot City*, we work in partnership to address these unfair differences in health.
Health starts in our communities. Community groups such as gardening clubs and singing groups are widely recognised as important cornerstones f community life. But the impact of these groups on community health often overlooked. Relationships between neighbours, community groups and trusted organisations are just as important for people’s health as the services we provide.
Community-centred approaches re central to our work to improve health in Leeds. We are proud to have long history of working in close collaboration with communities and CFS organisations. This made a real difference during the COVID-19 pandemic, where we could build on strong, trusted relationships to support communities. This way of working is strength of Leeds, which should be valued and celebrated. It builds the community resilience we need to face future challenges.
I have been inspired by the examples of brilliant work with and by communities that I have seen across Leeds – from Better Together groups providing friendship and skills, to Neighbourhood Networks supporting people in later life to stay active and connected. There are so many examples across the city to celebrate, and this report provides a small snapshot of them.
Leeds has a strong foundation for this work, with strong community assets and clear evidence that underpins good practice across the city. Building on this, the report sets out recommendations to support a system-wide commitment to strengthen and scale up community-centred working in Leeds.
Victoria Eaton. Director of Public Health
What is a Marmot City?
In Leeds, being a Marmot City means putting fairness and health at the centre of decision making so that everyone has the chance of a healthy life. This includes improving the ‘building blocks’ of good health, things like housing, education and community connections. It also means ensuring that service and resources are delivered at a level that meets people’s needs.
Contents
Foreword
Communities create good health and wellbeing
What do we mean by ‘community-centred’ approaches?
Communities at the centre of local and national strategy
Why do we work with communities?
There are inequalities in health between communities in Leeds
Working with communities is an effective way to improve health and wellbeing and reduce inequalities
Communities have assets to build on
How do we work with communities in Leeds?
The family of community-centred approaches
c) Collaborations and partnerships
Conclusion and recommendations
Update on recommendations in the 2025 DPH Report: Heat in the City
Background
Leeds is a large and diverse city, home to communities of people from different backgrounds, with different characteristics and interests.
We put communities at the centre of our approach to public health in Leeds. This means working with and for communities, rather than doing something to communities. This helps us improve health, keep people safe, and make sure everyone can access health and wider services. Leeds has been working this way for many years. Over recent decades, research has consistently shown that building strong, connected communities is a sustainable and effective way to improve health outcomes.
This report celebrates our work with communities and how it improves health and wellbeing and helps reduce inequalities in Leeds, including:
-
- Why we work in this way, including an explanation and summary of national and international evidence.
- Examples of brilliant work with communities that has made a difference.
- Recommendations to further improve this way of working in Leeds.
What is a community?
Communities share something in common. They give us a feeling of belonging and connection to others.
Community has been described as “the relationships, bonds, identities and interests that join people together or give them a shared stake in a place, service, culture or activity”
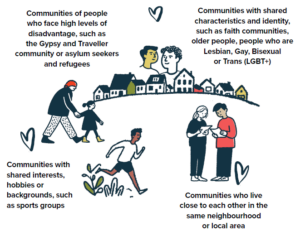
Illustration showing the following groups:
-
- Communities of people who face high levels of disadvantage, such as the Gypsy and Traveller community or asylum seekers and refugees
- Communities with shared characteristics and identity, such as faith communities, older people, people who are Lesbian, Gay, Bisexual or Trans (LGBT+)
- Communities with shared interests, hobbies or backgrounds, such as sports groups
- Communities who live close to each other in the same neighbourhood or local area
As this graphic shows, communities are complex. Most of us are part of several communities, and these change over time. As we get older and our lives change, we might move house, develop new identities or take up new interests. It is important not to place people into ‘boxes’ or talk about communities in isolation. People’s experiences and identities are shaped by many aspects of their lives.
What are health inequalities?
Health inequalities are avoidable, unfair and systematic differences in health outcomes, access to health care and opportunities for healthy living between different groups of people. These differences are not random. They are driven by inequalities in society, including income, education, discrimination and where people live.
Life in Leeds: Communities and assets in the city
All communities in Leeds have strengths and resources, often described as “assets”, that can support health and wellbeing. These include parks and green spaces, local services such as schools, and the knowledge and relationships held by VCFS organisations. Community-centred approaches recognise,
build on and strengthen these assets, especially where barriers exist.

Infographic showing various communities and assets as follows:
-
- 845,200 people live in Leeds
- Over 70,000 people in Leeds have a main language that is not English. For example, 4,697 speak Romanian, and 2,898 speak Kurdish
- Around 1 in 5 people (1 in 4 children, 1 in 10 older adults) live in the most deprived 10% of neighbourhoods nationally
- Around 1 in 10 people live in the least deprived 10% of areas nationally
- Around a quarter of people are from ethnically diverse communities
- 31,500 volunteers, and 6,465 employees working in 3,375 VCFS organisations
- 30 VCS Community Anchors
- 34 Neighbourhood Networks supporting older people
- 222 primary schools
- 40 secondary schools (and 4 through schools)
- 5 Further Education colleges
- 5 Universities
- 99 Councillors
- 250+sporting groups
- 87 GP practices
- 150+ established places of worship
Communities create good health and wellbeing
Health and wellbeing is shaped by the conditions people experience throughout their lives, including their homes, their work and their communities. People’s health improves when they feel connected, included and able to take part in decisions that affect their lives.
Communities can create a sense of belonging, build relationships and be a source of joy. This was clear during the COVID-19 pandemic, when neighbours supported each other by offering friendship, sharing food and providing practical help. Across the city, many people volunteer in their neighbourhoods, and communities are already taking action to improve health and wellbeing.
However, not all communities have the same access to these benefits. Some people experience discrimination, exclusion or a lack of power and control, which can limit opportunities to build connections and protect health. This is why trusted community organisations that work closely with communities play such an important role in improving health and reducing inequalities. Later in this report, we share examples of how organisations like these make a difference to health and wellbeing.
How people in Leeds feel about their communities
The Community Life Survey tells us how people feel about their communities and their role within them. In Leeds:
-
- 22% feel they can influence decisions in their local area
- 73% are satisfied with their local area as a place to live
- 54% have volunteered in the last 12 months
- 34% believe many people in their neighbourhood can be trusted
- 6% often or always feel lonely
- 78% agree that their local area is a place where people from different backgrounds get on well together
- People in Leeds are more likely to be satisfied with their local area and feel that people can be trusted than some other large cities.
Source: Community Life Survey 2024/25
What do we mean by ‘community-centred’ approaches?
We work with and for communities to make the greatest difference to health and wellbeing and reduce inequalities in Leeds. This is not just about being physically present in communities – it is about involving people in a meaningful way, and ensuring different groups are included. It recognises that people are experts in their own lives and best placed to define the solutions they need. This is particularly important for groups facing the greatest disadvantage and extreme health inequalities. Public health teams, local government, the NHS, VCFS organisations and other partners all have an important role to play as part of this.
“Communities know what they need and have the wisdoms and solutions to achieve change.” – Quote from the Listening Exercise
Community centred approaches are practical, evidence-based approaches that:
-
- use non-clinical, community-level approaches
- shape the building blocks of health
- increase people’s control over their health and lives
- actively involve community members throughout the process
- Community centred approaches
- improve connection and networks
- remove obstacles to involvement e.g. transport
Case Study
Leeds Community Anchor Network – connecting community organisations working to ensure the communities of Leeds thrive
The Leeds Community Anchor Network (LCAN) is a city-wide network of 30 trusted VCFS organisations. The network formed in 2022 to build on the connections and partnerships made during the COVID-19 pandemic. LCAN brings together organisations whose purpose is to ensure the communities of Leeds thrive, working in collaboration rather than competition. This includes:
- Delivering the Neighbourhood Matching Programme, which provides funding to projects chosen by local volunteers in return for their time volunteering. This programme shifts power to communities to set their own local priorities. In total, 46 volunteer-led projects have been funded through the time of 676 volunteers, raising £58,100. Projects have included residents spending time litter picking to fund new bins in Holbeck and volunteers growing and cooking vegetables in Seacroft.
- Co-ordinating the Welcome Spaces Network of local trusted organisations providing community spaces where people can gather for free in a warm, safe place and enjoy a hot drink and some company. Some provide activities and sessions, such as cooking. In winter 2024-25, 30 LCAN members co-ordinated a network of over 200 Welcome Spaces in the city, with 65,653 visits from residents
“Community is important. It is not about what is happening but the people forming connection with one another.” Quote from Welcome Space Provider
Communities at the centre of local and national strategy
Ensuring communities are involved and empowered, particularly those facing disadvantage, is central to strategies and approaches in Leeds.
In 2025, the Leeds Ambitions were launched by Leeds City Council and partners in the city, setting out four overarching ambitions for Leeds to be a healthy, growing, thriving and resilient city. Community-centred approaches will help deliver these ambitions. Key local strategies and programmes of work that support this include:
-
- The Joint Health and Wellbeing Strategy (2023–30)
- Our Leeds commitment to being a Marmot City
- Community power in the city, expanding on work to shift power to people and enabling communities to thrive
- The Third Sector Strategy (2023-2028) to ensure the VCFS is diverse, resilient and better able to continue supporting our communities
- The Leeds Volunteering Strategy (2023) celebrating and supporting volunteering.
In addition, new national directions provide opportunities for community-centred approaches and will have a significant impact on Leeds:
-
- In 2025, the new 10 year Health Plan for England was published, setting out a new approach to delivering Neighbourhood Health.
- The national Pride in Place approach, enabling residents, businesses, and community groups to deliver real improvements that matter to local people, will include four neighbourhoods in Leeds (Middleton Park Avenue, Farnley East, Seacroft, Armley and New Wortley).
Neighbourhood Health in Leeds
Neighbourhood Health is a partnership approach to delivering co-ordinated, accessible and preventive health and care services in a local community. Leeds is a national pilot site for Neighbourhood Health (National Neighbourhood Health Implementation Programme) in Chapeltown, Beeston, Middleton and Hunslet, Cross Gates and Seacroft. Learning from this will help develop Neighbourhood Health approaches across the city.
Why do we work with communities?
We use community-centred approaches because they help us meet the needs of Leeds’ many and diverse communities, and because there is strong evidence that they improve health and reduce health inequalities.
There are inequalities in health between communities in Leeds
Leeds covers a wide and varied geography, from urban areas to rural communities. This means that areas with high levels of deprivation often sit alongside more affluent areas. Neighbourhoods across the city have different characteristics, strengths and health needs.
People in more deprived neighbourhoods of the city are more likely to die earlier and be unwell for more of their lives. In the parts of Leeds within the most deprived 10% of England, life expectancy is 73.2 years (men) and 78.2 years (women), compared to 83.6 years (men) and 86.7 years (women) in the parts of Leeds in the least deprived 10% of England (ONS population and mortality data 2022-2024 and IMD 2025 at LSOA level). People living in the most deprived areas live around a third of their lives in ill-health, compared to less than a fifth in the least deprived areas (Healthy life expectancy data 2013-15 and 2020-22).
The most deprived neighbourhoods are younger, with more children and families, and more ethnically diverse. People from ethnically diverse communities may experience inequalities in health, the building blocks of health – such as housing, education and employment, and access to support and services.
People belong to multiple communities, all of which shape our health and wellbeing. For example, people living in the most deprived neighbourhoods are more likely to be from ethnically diverse communities, or people who are homeless may also have challenges with substance use. Together, these can have significant, overlapping impacts on health inequalities
Understanding Deprivation
Deprivation means not having the resources, opportunities, or living conditions necessary for a good quality of life and good health.
The Index of Multiple Deprivation (IMD) provides a picture of how deprived a neighbourhood is by using measures of daily life, including income, health and the local environment. The way deprivation is measured in England was updated in October 2025, so we cannot make a direct comparison with previous figures.
Life expectancy at birth 2022-24
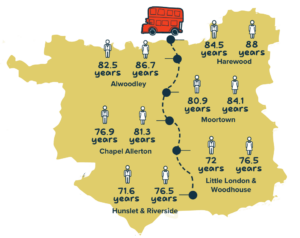
Image shows a map of Leeds with a fictional bus route from North Leeds to South Leeds. Ward level life expectancy at birth is shown for some wards as follows:
-
- Harewood: Males 84.5 years, Females 88.0 years
- Alwoodley: Males 82.5 years, Females 86.7 years
- Moortown: Males 80.9 years, Females 84.1 years
- Chapel Allerton. Males 76.9, Females 81.3 years
- Little London & Woodhouse. Males 72.0, Females 76.5 years
- Hunslet & Riverside. Males 71.6 years, Females 76.5 years
A baby born in Harewood can expect to live 12.9 years (men) or 11.5 years (women) longer than a baby born in Hunslet & Riverside.
Source: Wards, calculated using ONS MYE populations, and ONS mortality data.
Communities experiencing extreme health inequalities in Leeds
Some communities in Leeds face extreme health inequalities, such as people who experience homelessness, people with drug dependence, at risk migrants, the Trans community, Gypsy and Traveller communities, Roma communities, people with learning disability, street sex workers, people in contact with the justice system and victims of modern slavery.
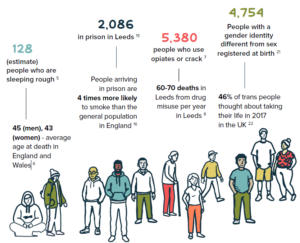
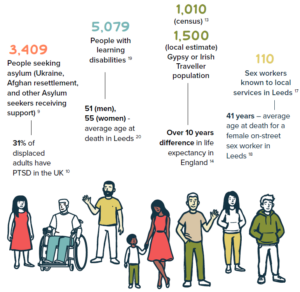
Infographic showing inclusion groups with some headline health statistics as follows:
-
- 128 People are sleeping rough in Leeds (estimate). Average age at death for people sleeping rough in England and Wales: 45 (men), 43 (women)
- 2,086 people in prison in Leeds. People arriving in prison are 4 times more likely to smoke than the general population in England
- 5,380 people who use opiates or crack. there are 60 to 70 deaths in Leeds from drug misuse per year in Leeds
- 4,750 People with a gender identity different from sex registered at birth. 46% of trans people thought about taking their life in 2017 in the UK
- 3,409 People seeking asylum (Ukraine, Afghan resettlement, and other Asylum seekers receiving support). 31% of displaced adults have PTSD in the UK
- 5,079 People with learning disabilities, average age at death in Leeds is 51 (men), 55 (women)
- Gypsy or Irish Traveller population in Leeds 1,500 (local estimate), and 1,010 (census). Life expectancy in England is over 10 years shorter
- 110 Sex workers known to local services in Leeds. Average age at death for a female on-street sex worker in Leeds is 41 years
People who face extreme health inequalities
Some communities in Leeds face extreme health inequalities, such as people who experience homelessness, people with drug dependence, at risk migrants, the Trans community, Gypsy and Traveller communities, Roma communities, people with learning disability, street sex workers, people in contact with the justice system and victims of modern slavery.
People in these communities often experience multiple, overlapping social and economic challenges, as well as stigma and discrimination. They have worse access to services, poorer health, lower quality of life, and shorter lives. For example, people who sleep rough die at age 45 (men) or 43 (women) on average. For several reasons, they are often missing from data records, so their needs may be ignored when services are being planned.
Work to address these inequalities is often called ‘inclusion health’. It focuses on the individual and their circumstances, including understanding and responding to the impact of trauma, and involving them in planning and delivery of services so that they meet their needs.
Note: Intelligence and data on many of these communities are not collected at national or local level. Therefore, many of their needs are hidden. Some data has only recently started to be collected, for example, ‘Roma’ ethnic heritage was only added to the census in 2021. There are many reasons for this, including barriers to accessing services, low levels of trust in statutory organisations and wariness of sharing personal details.
Working with communities is an effective way to improve health and wellbeing and reduce inequalities
There is strong and growing evidence that community-centred approaches improve people’s health and reduce inequalities. This is not a new idea – community participation and empowerment have been central throughout the history of public health and health promotion. But recent evidence has improved our understanding of how and why these approaches work.
Reducing health inequalities
Many communities face barriers to accessing health and wider services, including a lack of trust, stigma or discrimination, and communication challenges. Working with communities to develop culturally appropriate and effective ways of connecting with people can improve access to services and reduce health inequalities.
Health messages are more likely to be believed and have an impact when they are delivered by people in the same community or a trusted community organisation, in safe and familiar settings. Peer support approaches and volunteers can reach people who have not been supported by other services. Often, the person delivering the message can be as important as the message itself. For example, collaborative work with mosques, churches and faith-based organisations to deliver culturally-sensitive health programmes have led to improvements in health, including mental health and heart disease.
“A lack of social connection is one of the key mechanisms that create and perpetuate health inequities” Quote from World Health Organization
Supporting strong, connected communities
Social connection improves our health and wellbeing. Strong relationships help people to be more resilient and protect against poor health. In contrast, social isolation and loneliness can be very damaging to health. It can lead to a higher risk of heart disease, stroke, and mental ill health. It has also been estimated that loneliness increases the chance of death by 26%. This is comparable to well-known risks to health such as smoking or obesity.
There is good evidence on what works to build social connection, reduce loneliness and improve health. Community groups such as gardening clubs, walking groups and women’s groups have often been thought of as “nice to have” in communities, but have in fact been shown to improve social connection and make a difference to health
Enabling voice and greater control
Having a voice in local decisions is important for people’s health and wellbeing. Existing services do not have all the answers. When organisations work in partnership with communities, more people can access support and health outcomes improve.
However, community involvement needs to be meaningful. This means not just providing information or running a consultation, but working together and shifting power and control to communities. The more the community is involved in joint decision making, the more embedded and successful the solution is likely to be. This is often referred to as ‘Community Power’, and there is a strong history of working in this way in Leeds, putting people at the heart of decision making in the city.
Community Power
Community Power means the transfer of power and resources to communities so that they can have greater influence and control over the plans, decisions, and public services that affect their lives. This reflects the belief that, given the tools and the opportunity, those who are part of a community can change the things that they believe need changing in their community better than anyone else.
Healthwatch Leeds
Healthwatch Leeds is an independent organisation that listens to people’s experiences of health and social care services. They make sure people’s voices are heard and at the heart of shaping health and care services in Leeds.
A ladder of participation

Infographic showing five steps as follows:
-
- Supporting local initiatives ‘We can help you achieve what you want, within guidelines’
- Acting together ‘We want to carry out joint decisions together’
- Deciding together ‘We want to develop options and decide together’
- Consultation ‘These are the options what do you think?’
- Information ‘Here’s what we are going to do…’
Learning from the COVID-19 pandemic
The COVID-19 pandemic shone a light on the value of communities for health and wellbeing. Communities and local organisations responded rapidly to provide support to people who were isolated or excluded. Support ranged from neighbours looking out for each other to co-ordinated emergency provision by VCFS organisations.
Trust was central. Globally, countries with higher levels of trust had higher rates of vaccination and lower rates of COVID-19 infections. In the UK, local approaches with communities, understanding beliefs and building sustained, trusting relationships were key to improving vaccination rates .
For example, approaches that included working with communities and culturally appropriate resources were more effective than incentives and mandates at engaging ethnically diverse populations. Community champion approaches were a widely used, effective approach to increase vaccination and support diverse and disadvantaged communities.
Case Study: Community Champions – local volunteers sharing trusted information and promoting health
Community Champions are local volunteers who draw on their own experience to share trusted information about services with people in their communities. Evidence shows this approach is especially effective in communities where trust in public services is low.
The Leeds Community Vaccine Champions programme is delivered by Forum Central and Voluntary Action Leeds, in partnership with Public Health, West Yorkshire Integrated Care Board and NHS England. Volunteers work with their local communities to improve understanding of vaccination, particularly in areas with lower uptake. Small grants support local, grassroots groups to take part. The programme builds on trusted ways of working developed during the COVID-19 pandemic.
Since the pandemic, more than 300 Community Champions, speaking over 40 community languages, have been active across Leeds. Champions have had more than 5,000 conversations with people from diverse communities. An ongoing evaluation has found the programme to be effective at raising awareness through informal community networks and supported vaccine pop-ups. This is thought to be a key factor in improving vaccination rates.
“You can spend thousands and millions on… printing out things and giving them to people. But nobody’s gonna have a look and they’ll just go straight in the bin. But you have one meaningful conversation and that lingers. And then that next person will end up saying it to somebody else.” Quote from Volunteer, Community Champions.
Communities have assets to build on
All communities have assets: the people, places and resources within a community that help protect and improve health and wellbeing. These can include local VCFS organisations, transport links, and green spaces such as parks. These are only community assets if the community itself says they are.
Not all communities have the same access to local assets, which affects health unequally. For example, people living in some deprived, central neighbourhoods may have strong community cohesion and VCFS organisations, but limited access to green space.
We have developed the Leeds Asset Framework to understand the different assets communities have available to them. These are grouped into:
Local services. Services provided by the health system, council, businesses or others, e.g.
-
- Health & care services including GP surgeries
- Schools
- Libraries
- Housing services/supported housing
- Transport services
- Businesses
- Other services
People and communities. Skills and knowledge in the community, e.g.
-
- Community knowledge and skills
- Friendships, good neighbours, and social networks
- Community spirit/cohesion
- Volunteering
- Local groups and networks (informal and formal)
- Local VCFS organisations
- Councillors and community leaders
Places. Buildings, infrastructure and green space, e.g.
-
- Environment and green space e.g. parks
- Community centres /hubs
- Housing
- Local economy and jobs
- Getting around – walking, cycling, transport
- Places of worship e.g. mosques/churches
- Shops and amenities
- Culture and history
Asset-based approaches – building on the strengths of communities
Asset-based approaches focus on what is strong in communities, not just on what is wrong. When we focus only on needs or problems, we risk labelling and stigmatising people. Building on community assets helps create the conditions for better health and fairer outcomes.
Asset-Based Community Development (ABCD) is a neighbourhood approach to community development. It brings people together around shared action to bring about change. ABCD recognises the strengths in communities, and that everyone has skills and something to contribute. It makes visible the strengths that are often invisible in communities. This is a shift to a bottom-up approach, run by the community themselves.
The five principles of ABCD are:
-
- Citizen driven
- Relationship oriented
- Asset-based
- Inclusion-focused
- Place-based
How do we work with communities in Leeds?
A foundation of working with communities
Leeds has a long and proud history of working with communities to improve the health of residents. Trusted partnerships built up over years of working together, investment in resources, and other community assets have enabled community-centred approaches to become established across the city.
In recent history, strong relationships with communities and VCFS organisations – particularly the Community Champions – were the foundation of our response to the COVID-19 pandemic in Leeds.
Vaccination centres in community locations improved uptake and reduced inequalities. For example, more than 50,000 doses of the COVID-19 vaccine were delivered at the Bilal Centre vaccination clinic in Harehills. The Leeds Vaccination Bus allowed for a community outreach approach to deliver vaccinations within areas of low uptake, providing 4,146 vaccinations for 2,854 individuals. And the Leaving No-One Behind work programme was established to overcome inequalities in vaccination uptake through approaches including women only sessions and workplace vaccination programmes.
We learned a great deal during the pandemic about our communities and the barriers they face in accessing healthcare. This learning continues to shape the way we work today.
“It’s the basic principles of Community Development, starting where people are, rather than where you want them to be, going at their own pace, listening, and respecting what they say” Quote: Pat McGeever, Health For All
The family of community-centred approaches
In 2015, Public Health England published a national guide to community-centred approaches. It includes the family of community-centred approaches that provides practical ways to improve health and wellbeing in communities. It is a way of identifying evidence-based options that are also rooted in public health practice.
The family of community-centred approaches outlines four practical ways to improve health and wellbeing using community assets and strengths to give people more control over their health and lives:
-
- Strengthening communities: Communities use their assets and strengths to work together to improve health and address the factors that affect it
- Volunteer and peer roles: Communities build skills and confidence so they can share advice, give support, and organise health and wellbeing activities in their own communities
- Collaborations and partnerships: Bringing together communities and local services to identify needs and priorities, plan and deliver activity that keeps them healthy
- Access to community resources: Connecting people to practical help, group activities, and volunteering activities
Source: Adapted from PHE (2015)
On the following pages we describe each area of the ‘family’, with case studies of projects and approaches in Leeds. It is important to note that projects do not always fit neatly into just one of the four approaches, but can showcase multiple elements.
a) Strengthening communities
These approaches strengthen communities to take collective action which will improve health. Examples of activities in Leeds to strengthen communities include capacity building, community health development programmes, ABCD and community organising and social network activities.
Public health plays an important role in identifying where there are fewer opportunities for collective action for particular communities, and works in collaboration to strengthen them.
Case Study. Better Together – trusted community health development
Better Together is a community health development service, commissioned by Public Health. It works with communities to develop and design approaches together to improve health and wellbeing and reduce social isolation.
The service engages over 10% of residents in Leeds’ most deprived areas (around 20,000 people annually) through outreach in everyday settings – such as community galas, workplaces, and community centres. There are over 2,000 local group activities, which are shaped by community priorities and include cooking, physical activity, peer support, employment, education, and arts.
“I love this group, I’ve made friends, it makes me so happy.” Quote from group participant, Better Together programme
Better Together effectively engages with diverse communities at risk of significant health inequalities, including people who might not use services. Public Health teams work with Better Together providers, building on their insight and trusted relationships to develop approaches that will work in different communities. The difference it makes to people’s health is measured with validated methods.
“Having welcoming spaces in communities is very important. It’s not just about the building – it needs to be a safe and warm place you want to go,” Quote from Helen Hart, Chief Executive of BARCA.
Better Together is delivered by grassroots organisations across Leeds: BARCA (West), Health for All, Asha, Holbeck Together, St Luke’s Cares (South), and Feel Good Factor, Shantona, Space 2, and Touchstone (East). These groups reflect and respond to local needs.
“Today I have a Doctor’s appointment, for the first time I am now going to go without an interpreter because I can go myself and understand.” Quote from group Member, Conversational English
Case Study. Neighbourhood networks – supporting people to live independently in their communities
Across Leeds, 34 locally-led Neighbourhood Networks support older peoples’ health, independence and community participation by providing a range of healthy living and social activities. Between April and June 2025 there were 103,172 instances of people attending the 751 activities.
Neighbourhood Networks increase social contact, reducing isolation and loneliness. They provide a range of healthy living activities, so that older people can maintain their independence, which also keeps them healthy. Network members spot if people’s health declines, helping them to get support early and reduce the need for health and care service interventions.
Armley Helping Hands (AHH) is a Neighbourhood Network in Armley, one of the most deprived wards in the city, with health challenges including healthy living (inactivity, overweight and drinking at higher risk levels), A&E admissions for falls, frailty, and social isolation.
Dawn Newsome, the CEO from AHH, talks with pride about the support, friendship and trust: “Last year we provided activities including peer support and education to manage long term conditions (we reached 1,300 people), support with food and nutrition (962 people), support around cost of living and finances (549 people) and one to one support and advice (161 people). We provided transport to ensure members can access sessions.”
b) Volunteer and peer roles
Volunteer and peer approaches enable people to use their skills and life experiences to support others in their community. These roles are usually taken on by local residents, who receive appropriate training and support. When support comes from people with shared experiences or identities, it can help break down barriers and build trust. Peer and volunteer roles include community health champions, befriending schemes, care navigators and peer supporters.
Many volunteers across Leeds contribute to health and wellbeing in their communities. Public Health supports people to become peer supporters or volunteers, with a focus on making sure people from different backgrounds and with different experiences have opportunities to take on these roles.
“Thank you to Armley Helping Hands for helping me see the light at the end of the tunnel, I was so negative on life when I first met the team, they have opened so many doors for me and given me back my independence and to have a meaning in life” Quote form service user, Helping Hands
Case Study. Migrant Community Networkers – trusted links between communities and services
Migrant Community Networkers are volunteers from migrant communities in Leeds who act as trusted links to services.
The network is hosted by the Migrant Access Project team in Leeds City Council, in partnership with Public Health and Leeds Health Awareness. Migrant Community Networkers share key health messages on topics such as vaccination, healthy living, long-term conditions and cancer. Networkers receive small grants to run workshops and share information creatively within their communities.
In 2024, 13 Networkers from countries including Eritrea, Jamaica, Iraq, Nigeria and Syria delivered 16 events on cancer and heart disease in nine languages, reaching at least 372 people. Networkers with shared backgrounds and languages were able to develop trust and hold conversations on sensitive topics through creative activities.
Feedback showed attendees felt more informed and motivated about risks, symptoms, and the importance of health checks and screening. Networkers also reported benefits to themselves, including increased confidence and experience for job applications.
“I never realised that catching cancer early could make such a difference. I’ll definitely go for my screening now.” Quote from community member, Migrant Community Networkers
Case Study. Drug and alcohol peer support – bringing lived experience to champion and support recovery
Leeds is part of an international movement of Inclusive Recovery Cities which increase the visibility of recovery, reduce stigma, and give hope to those struggling with addiction and their families.
Peer-led recovery activities take place across the city, supported by Public Health. The 5 Ways Recovery Hub (part of Forward Leeds, the city’s drug and alcohol service) is a vibrant community offering peer support and activities to challenge boredom and promote social connection. Independent peer-led recovery organisations such as Getting Clean CIC, Sober Butterflies, and Recovery Runners, run a wide range of activities such as running, climbing, soap making, community clean-ups, and gardening.
Recovery communities build social connection and a sense of community, provide support, enable people to have fun and develop skills, enhance feelings of self-worth, and prevent relapse. Volunteers and peers share important life experiences, so they can understand, inspire and support others on treatment and recovery journeys.
In the last six months, Getting Clean CIC has made 6,000 bars of soap, with 150 volunteers (of which six were employed), with positive recovery and broader health impacts.
“Getting involved gave me purpose and built my confidence, whilst building a support network of friends in recovery.” Quote from participant, Getting Clean CIC
c) Collaborations and partnerships
When we work in partnership with communities and local organisations, we hear important ideas and information from different groups and sources. This helps us work in an effective, inclusive way so that services are better aligned with local needs, and decisions are informed by community insight.
The Public Health team recently completed assessments of the health needs and assets in neighbourhoods in the city in collaboration with local communities. These assessments bring together data and evidence on health with the voices of community members, including ideas for solutions. This in turn informs partnership work to improve health and wellbeing and reduce inequalities.
The case studies on the next page show how collaborative working in Leeds supports joined-up approaches to health.
Case Study. Local Care Partnerships – joined up, holistic care in communities
Local Care Partnerships (LCPs) are partnerships between the NHS, Leeds City Council, VCFS organisations and elected members. People work together across organisations to deliver joined-up, collaborative care that meets the needs of local communities.
There are 15 LCPs covering the whole of the city, tailored to local community needs and characteristics. Some examples of LCP work include:
-
- An LCP in East Leeds identified domestic violence and abuse as a priority and took a ‘whole neighbourhood approach’ to addressing it. Activities completed include a theatre production attended by 300 young people, training on domestic violence and abuse and honour-based violence, training of 31 domestic violence and abuse ambassadors in the community, and a range of workshops and lunch and learn sessions.
-
- An LCP in Inner West Leeds identified healthy eating for families as a local priority and developed fun, free local community projects to support families in inner city areas, including family cooking clubs and courses to cook healthy, affordable meals at home. An LCP in North East Leeds developed whole workforce training to improve confidence in supporting people around healthy eating.
Case Study. The Listening Project – listening to communities across the city
In 2024, Leeds Community Anchor Network organisations conducted community listening activities in all wards of the city, with additional activities in the areas with the highest levels of deprivation.
Listening exercises provide the opportunity to hear from local communities on what they value about where they live, what they see as strengths and assets in the community, and ideas for changes, including:
-
- What’s great about your area?
- How could it be better?
- What could it look like in 10 years?
A total of 1,958 people completed a postcard exercise and 529 took part in focus groups. Most responses were positive, with people saying they valued strong community spirit, green spaces, and local community organisations and activities. Priorities identified included community safety, improving parks and green spaces, youth activities, transport and cleaner streets.
Findings are being used to shape how local organisations work with communities, including supporting communities to take action themselves based on understanding of local needs and strengths.
“One of the most beautiful findings in The Listening Project is the love — the genuine, powerful love — that people in Leeds have for their communities. Again and again, we heard about strength, about pride, about deep connections. People told us what they value most about where they live, and it turns out there is so much to celebrate.” Quote from Howard Bradley
Listening project feedback – ‘What’s great about your area?’
Armley:
-
- Community spirit and togetherness
- Green spaces
- Community activities
- Educational facilities
Beeston:
-
- Community spaces
- Community spirit and togetherness
- Green spaces
- Diversity
Gipton:
-
- Green spaces
- Community spirit and togetherness
- Shopping
- Transport
Hunslet & Riverside:
-
- Community spirit and togetherness
- Local charities/organisations
- Diversity
- Green spaces
Burmantofts & Richmond Hill:
-
- Community spirit and togetherness
- Green spaces
- Community activities
- Proximity to town
Harehills:
-
- Healthcare
- Local charities/organisations
- Religious buildings
- Educational facilities
Holbeck:
-
- Community spirit and togetherness
- Local charities/organisations
- Community spaces
- Community activities
Killingbeck & Seacroft:
-
- Community spirit and togetherness
- Green spaces
- Local charities/organisations
- Shopping
d) Access to community assets
Not all communities have the same access to community assets that can improve health and wellbeing. Even where strong community assets exist, some people may face barriers to access them, including lack of information, confidence, transport or trust.
This is why we have established approaches to connect people to community assets and practical help, such as community hubs, community navigators and social prescribing.
Evidence shows that trusted roles can help people to connect to local assets. For example, Community Health and Wellbeing Workers are trained peers who build relationships, offer support, and help people access health services, with positive outcomes including increase in cancer screening and vaccination rates.
Public Health has an important role to understand where people face barriers to accessing community assets, and to work with communities to remove these barriers so people can get the support they need. This can include investing in local infrastructure and developing assets such as libraries and community anchors that support connection.
Partnership with community organisations to support groups who face extreme health inequalities
Public Health works in close partnership with community organisations to support people facing extreme health inequalities to ensure that they benefit from services in Leeds.
The following three case studies – with the Gypsy and Traveller community, rough sleepers, and women who are sex working – show how different community partnership approaches can support different groups.
Case Study. Health and wellbeing support with the Gypsy and Traveller community
Leeds Gypsy and Traveller Exchange (GATE) is a trusted local organisation who work for and represent the needs of the Gypsy and Traveller community. The GATE Health and Wellbeing service is commissioned by Public Health. It offers group sessions on topics chosen by members, such as isolation and loneliness, and provides support with accessing health services. Sessions are often creative, for example making healthy food or flower arranging. Some of the GATE members have become Health Champions and deliver sessions themselves to support their peers. Training is provided to help develop new skills and interests, which they then share with the group.
There were 656 instances of Gypsy and Travellers attending GATE during 2024-2025. Participants reported improved mental wellbeing, feeling less isolated and an enhanced sense of belonging.
“I didn’t take the role as a Health Champion serious at first but then when I started getting more involved, I could see my skills improving and my confidence. This helped me to apply for a role that came up and to get the job. I can now see how having some involvement even if it’s only small can really make a difference and leads on to further opportunities”. Quote from employee and former Health Champion, GATE
Case Study. Drug and alcohol support for rough sleepers
The Rough Sleepers Team (part of the Forward Leeds drug and alcohol service) provides rapid access to drug and alcohol treatment and links people to wider health and practical support. They build relationships and work in a way that is sensitive to the traumas that people may have experienced.
In 2024/25 the team supported 119 people in Leeds. GW, a 54-year-old man, lived with addiction for over 40 years. He connected with the Rough Sleepers team after he was released from prison. He completed drug detox and rehab and now lives in permanent housing in Scarborough, volunteers in a charity shop, and shares his story with people in Leeds to support and inspire them. GW shared a photo of himself enjoying ice cream on the beach.
Case Study. Support for women who are sex working in Leeds
Basis Leeds provides health care and support for women who are sex working in Leeds, focusing on those most at risk, commissioned by Public Health and other partners. They provide support in the places where women live, working from a van and trusted community locations. They work with the Leeds Sexual Health service to provide condoms, vaccination, screening and treatment, along with wider support on housing, finances, drugs and other issues. Basis worked with 271 people last year, many of whom never access other services and support in the city.
The team develops trusted relationships that are non-judgemental and sensitive to trauma that people have faced. Women have a choice over how they are supported and control over the changes they want to make in their lives. They tap into the interests, skills, and experience of the women to improve confidence and support people to enter training, volunteering or employment.
Case Study. Linking Leeds – social prescribing transforms care to address the root causes of poor health
Linking Leeds connects people to activities and support in their community and reduces demand for medical appointments. It is a vital part of the city’s health and care system, commissioned by the Integrated Care Board and delivered by a consortium of VCFS organisations. It offers time and support to anyone aged 16+, anywhere in the city, including those not registered with a GP. It works alongside social prescribers employed by GP surgeries.
When people use the service, they work with a wellbeing co-ordinator to develop a plan, which takes a holistic view of the person to address things such as social isolation, housing and financial stress that can affect people’s health. Wellbeing co-ordinators have deep local knowledge and relationships with VCFS and statutory partners, which makes them uniquely positioned to support people holistically.
A recent evaluation found that people significantly reduced health service use, including a 92% probability that someone will attend the GP less frequently, after receiving support from Linking Leeds, after receiving support from Linking Leeds. Improvements are seen for all age groups using validated measures, with the greatest gains in younger people, those from deprived areas, and women.
4. Creating the short film
To accompany this report, we produced a short film. The film highlights the work being done across our city to take a community-centred approach to people’s health, as well as the need for this work.
Over two days, we visited a selection of community-based projects across Leeds that are working to improve people’s health and wellbeing. We spent time with people who attend the groups run by these projects, those who organise and support them, and organisations delivering this vital work on the ground. We also spoke with one academic whose research focuses on community-centred approaches to health, helping to situate these lived experiences within a wider evidence base.
The film reflects a broad mix of people, places and perspectives, but it does not aim to be exhaustive. Leeds is home to many community-led projects doing impactful work, and while we have spoken with many of these partners during the creation of this report and film, we have only been able to highlight a small number of these as illustrative examples. Together, the report and film offer insight into how community-centred approaches are contributing to healthier lives across the city.
5. Conclusion and recommendations
Our communities create good health in many ways, from everyday acts of neighbourliness to collaboration between services and communities. During the COVID-19 pandemic, action by communities and longstanding relationships with local organisations made a difference to health outcomes for communities across the city.
They are now central to our city’s resilience and response to future challenges.
There is a lot that we should feel proud of as a city. But there are also opportunities for improvement, learning and better embedding of good practice throughout the system. The importance of trust was a thread throughout this report, and models including volunteer and peer roles play an important role to reach all communities and reduce health inequalities. The lack of intelligence and insight on groups facing extreme health inequalities hinders tailored, appropriate and effective approaches to address these inequalities.
The health challenges and inequalities faced by communities in Leeds cannot be solved by services alone. Community-centred approaches offer an effective, equitable way to improve health and wellbeing and reduce inequalities. They are not an alternative to clinical services; they are an important complement to ensure we reach all communities. They make a difference to health behaviours, access to services and better and fairer health outcomes – particularly for those communities experiencing the greatest disadvantage.
Key messages
These are our priorities to strengthen community-centred approaches for health. We believe these will help shape better and fairer health outcomes across the city.
-
- Start with communities: Start with the strengths, assets and needs of the community and build from there. Tailor approaches, think holistically about people and meet them where they are.
- Central to all our work: Community-centred approaches are not a single project or intervention. They are woven through all our work to improve health and address inequalities.
- Recognised and valued: Protect community-centred approaches as an effective, fair approach. Learn from projects that make a difference and scale them up to increase impact.
- Long-term investment: Building trust and community capacity takes time. It requires sustainable approaches and investment to build lasting impact, rather than one-off, short-term funding.
- Trust is key: Trusted relationships with communities and VCFS organisations are essential. They are part of our health and wellbeing infrastructure and are critical to our preparedness for future health emergencies.
- Meaningful collaboration: Engaging with communities in a meaningful way means sharing decision-making and trusting communities. Community priorities may not always align with our priorities, but working in this way helps to build trust and deliver outcomes.
- Prioritise communities facing extreme health inequalities: Effective engagement with communities and improved data collection and analysis are needed to develop tailored, effective approaches.
Recommendations
We have developed eight recommendations to build on strong foundations in Leeds to and have an impact on better and fairer health outcomes. The recommendations are relevant for work from birth through to older age and require a joined-up approach across public health and other parts of LCC, NHS organisations, VCFS and academic partners.
-
- Leeds City Council and academic partners to develop a simple guide to support assessment and improvement of community-centred approaches to improve health across the city.
- Leeds Health Protection Board to ensure community centred approaches are central to outbreak and pandemic planning, drawing on local experience and learning. This includes adopting sustainable approaches to community champions for long term impact.
- Leeds City Council and NHS organisations should aim for sustainable, long-term contracts and approaches with the VCFS in recognition of their critical role in delivering community-centred approaches to improve health.
- Leeds City Council, NHS organisations and VCFS to scale up community-centred approaches that work through all parts of the system, in line with Marmot principles. This includes new programmes such as Neighbourhood Health.
- Leeds City Council, NHS organisations and VCFS to explore opportunities to strengthen peer and volunteer roles as a practical approach to build trust and address health inequalities.
- Leeds City Council and NHS organisations, in partnership with VCFS, to ensure people facing extreme health inequalities are included as a priority through all parts of the system. This includes new programmes such as neighbourhood health.
- Leeds City Council Public Health Intelligence, NHS organisations and VCFS to identify and implement opportunities to improve intelligence, insight, analysis and reporting on groups facing extreme health inequalities. This is to provide robust reporting of health inequalities and the impact of work to reduce them.
- Local academic sector to strengthen local research and evaluation to inform programmes and services to improve health and wellbeing and reduce inequalities. This includes understanding communities’ strengths and needs, learning from community-centred approaches, and involving communities in research.
6. Update on Recommendations in the 2025 DPH Report: Heat in the City
This section provides an update on progress on the recommendations from last year’s report.
- Leeds City Council, Leeds Health and Care Partnership, anchor organisations and third sector to work collaboratively to promote and implement the advice and actions in the UK Health Security Agency (UKHSA) Adverse Weather & Health Plan
-
- Seasonal weather health bulletins are now issued to 550+ partners to strengthen city-wide preparedness.
- A cross-directorate approach is now in place to cascade UKHSA alerts through Essendex and Leeds Prepared Facebook for timely public updates.
- Continued investment in Beat the Heat resources for public, frontline staff and high-risk groups, including heat-illness guidance and home temperature monitoring.
- The Leeds NHS Net Zero working group is progressing recommendations on built-environment improvements, staff training and public messaging.
- Primary care health inequality templates are being updated with heat-risk prompts for identification and advice.
- Social determinant read-codes now include affordability of seasonal clothing and weather-affected living conditions (damp, mould).
- Leeds Water Safety Group has strengthened co-ordination of adverse-weather messaging.
- Weather and climate factors have been embedded into the Leeds Neighbourhood Health Model to target population-level interventions.
2. Leeds City Council, Leeds Health and Care Partnership, anchor organisations and third sector partners to work collaboratively to further improve access to cool spaces across the city by:
-
- Building on and promoting Leeds cool spaces guidance with partners and increasing public awareness.
- Ensuring there is a fair spread of cool spaces according to need across the city including community venues and seating in shaded areas.
- Public Health and Financial Inclusion teams are piloting a Leeds Cool Spaces Network for Summer 2026 using community hubs, libraries, neighbourhood networks and potentially health centres.
- Hydration stations and refill points are being explored, aligned with Cool Spaces messaging.
- We are currently exploring how to integrate cool-space principles into Age & Dementia Friendly and Come in and Rest venues.
- We are collaborating with Climate, Energy and Greenspaces teams to support natural shading within current and future green space developments.
- Heat-responsive adaptations (timing, venue choice, cool spaces, water availability) will be reflected in future procurement cycles for key public health contracts.
3 Leeds City Council, Leeds Health and Care Partnership, and Third Sector partners to work together to review and increase opportunities for community engagement around the health impacts of increasing heat through the development of a city-wide action plan.
-
- The Thackray Museum of Medicine exhibited the Heat in the City film with information boards and an interactive activity to collect public experiences of heat.
- Leeds Climate Emergency Advisory Committee is supporting delivery of the action plan and disseminating public-facing messages via elected members.
- Regular engagement with Health & Wellbeing Champions is raising the profile of heat risks among elected members and communities.
4 Academic partners to support city-wide work to strengthen local research, evidence and evaluation in relation to urban-heat mapping and climate vulnerability tools.
-
- SHIELD study: A University of Leeds project is developing tools to help care homes and home care apply heat-mitigation guidance.
- UrbanCool bid: Joint Leeds partnership on heat-resilient infrastructure, green space and preparedness (decision due early 2026).
- The Ageing Well team is working with the University of Leeds on research into seasonal use of urban green spaces by older adults and the barriers to access.
- Public Health are collaborating on the development of technology-enabled care, including falls prevention, indoor temperature tracking and hydration monitoring.
5. Leeds City Council will ensure that heat and health is considered in planning, particularly within densely populated inner city areas by ensuring:
-
- That planning applications are informed by ward-specific heat data.
- Health Impact of heat is included in health needs assessments.
- Continued development of design guidelines for green spaces that are adaptable to the changing climate.
- Discussions are underway with LCC Planning and Sensing Leeds to strengthen heat resilience in policy and guidance.
- The provision of natural shading is being considered within new developments, including the Heart of Holbeck project.
- Heat-related questions are now to be considered as part of the Health Impact Assessment used in planning processes.
- Draft Street Café Licensing guidance includes considerations and messaging related to heat impacts
6. West Yorkshire Combined Authority and Leeds City Council will continue to work together to:
-
- Identify opportunities for funding and investment in energy efficiency measures within Leeds housing stock.
- Lobby for improvement in national policy around rental housing to ensure landlords are responsible for making improvements that protect against heat as well as cold.
- Promote energy-efficient, climate-resilient housing.
- The new Warm Homes Local Grants Scheme (2026–28) will highlight the cooling benefits of thermal efficiency.
- We work with Home Plus Leeds to improve communication on how energy-efficiency measures help keep homes cool and to expand practical support.
- Review of the Good Home Hub included guidance and support on keeping homes cool.
- Public Health are working with housing and extra-care teams to ensure staff can support at-risk residents during periods of high heat.
7. Leeds City Council, Leeds Health and Care Partnership, Anchor Organisations, Third Sector and local businesses to work collaboratively to consider increased risk of vector borne diseases and heat for outdoor workers/workers at risk.
-
- In summer 2025 Leeds City Council ran a social -media campaign on tick awareness and prevention.
- Tick-awareness posters will be present in all parks from Spring 2026, as well as materials for garden centres and landscape suppliers.
- A partnership is in place with Leeds Anchor Network Climate subgroup to share UKHSA tick and heat-safety guidance with private-sector outdoor workers.
8. Health and Wellbeing Board to continue to address health inequalities via the Fairer, Healthier Leeds (Marmot City) and other health inequalities work. Address health inequalities through Marmot City work
-
- A new group has been formed to maximise the health impact of selective licensing, including focus on heat and cold.
- The Heart of Holbeck project is trialling the Health Equity Assessment Tool to influence design; recommendations include adding heat-related questions to consultation.
9. Leeds City Council, Leeds Health and Care Partnership, anchor organisations, and third sector partners to develop skills and knowledge amongst frontline workforce in protecting people at increased risk from the adverse health impacts of heat. Increase frontline workforce knowledge and skills
-
- The Weather Health Improvement Group continues to provide heat-related training and resources.
- Joint Public Health, ASC and RET workshops have been delivered on heatwave preparedness for care home and home care managers.
- Discharge teams across acute, community and adult social care services have been trained in MECC-based weather-health messaging, improving preventative advice and reducing the risk of heat-related readmission.
Acknowledgements
Thank you to all those who have contributed to this year’s annual report.
Writing Team:
Authors, editors and project management, data and intelligence: Pippa Bird, Lizzie Dawson, Quenby Harley, Nicola Kelly-Johnson, Chetna Patel, Adam Taylor, Tim Taylor, Frank Wood
Academic collaborators
Jane South, Leeds Beckett University
Jude Stansfield, Leeds Beckett University
Organisations and individuals who contributed to the report and provided insights for case studies:
Jon Hindley, Leeds City Council
Catherine Ward, Leeds City Council
Mindy Grewal, Leeds City Council
Magdalena Boo, Leeds City Council
Dan Burn, Leeds City Council
Lucy Insam, Leeds City Council
Kerry Swift, Leeds City Council
Kate Daly, Leeds City Council
Louise Cresswell, Leeds City Council
Chloe Rankin, Leeds City Council
Ololade Olaleye, Leeds City Council
Leisa Batkin, Leeds City Council
Helen Laird, Leeds City Council
Dawn Newsome, Armley Helping Hands
Kim Adams, LCP Development Team
Rachel Ainscough, LCP Development Team
Howard Bradley, LS14 Trust
Hannah Taylor, Sober Butterflies
Gemma Sharp, Getting Clean
David Best, Star Recovery
Sue Northcott, 5 Ways Recovery Hub, Forward Leeds
Mark Hindwell, Forward Leeds
Chris Sylvester, Getting Clean
Bill Owen, BARCA
Anna Martin, Voluntary Action Leeds
Bernie Gahan, Leeds Mencap
Pip Goff, Forum Central
Filming locations:
Feel Good Factor, Chapeltown
Beeston Village Community Centre, Beeston
Health For All, Middleton
St Agnes Church, Burmantofts
Leeds Gypsy and Traveller Exchange (GATE), Cross Green
Hawksworth Older Peoples Support Service (HOPS), Hawksworth
Space2, The Old Fire Station, Gipton
Photography and filming:
Brightsparks Agency
With thanks to all the organisations, groups and partners across Leeds who shared photography and filmed content for this report, helping to showcase the fantastic work they deliver in communities.
People and organisations who contributed to the film:
Staff, volunteers and attendees of the Feel Good Factor Arts & Crafts Group
Staff, volunteers and attendees of Beetey Din Lunch Club (Health for All),
Staff and volunteers at the Beeston Village Community Centre Food Pantry (Health for All)
Pat McGeever, CE, Health for All
Balwinder Kaur, Healthy Communities Manager, Health for All
Staff, Attendees and Community Champions at Voluntary Action Leeds and Forum Central Vaccine Community Champions Event.
Staff at Leeds Gypsy and Traveller Exchange (GATE)
Staff, volunteers and attendees at BARCA Leeds’ Conversation Café
Paul Barker, Co-Director Projects and Partnerships, Space2
Staff at Space2
Facilitators of Brave Words Drama Group at Space2
Professor Jane South, Professor of Healthy Communities at LSBU
Dean Matheson, Director, Calm & Centred CIC
Further Reading
Public Health England (2015) A guide to community-centred approaches for health and wellbeing
Public Health England (2020) Community-centred public health Taking a whole system approach Briefing of research findings
Health matters: community-centred approaches for health and wellbeing
Community-centred public health: Taking a whole-system approach
World Health Organization (2025). World report on social determinants of health equity.
Marmot M (2010) Fair Society, Healthy Lives. The Marmot Review
Bagnall A.M., Southby, K., Jones, R. et al. (2023) Systematic review of community infrastructure (place and space) to boost social relations and community wellbeing: Five year refresh.
If you need information from this report in a different format, please email: publichealth.enquiries@leeds.gov.uk
Please tell us the web address (URL) of the content, your name and email address and the format you need. For example: audio, braille, BSL or large print.
Further information on health statistics for Leeds and past reports are available online at:
https://observatory.leeds.gov.uk/dph-report/
We welcome feedback about our annual report.
If you have any comments, please email: publichealth.enquiries@leeds.gov.uk
Report Design: Brightsparks Agency
© Copyright Leeds City Council 2026
Creating better health together in Leeds